Genetic test for lactose intolerance A practical alternative
Pathomechanism
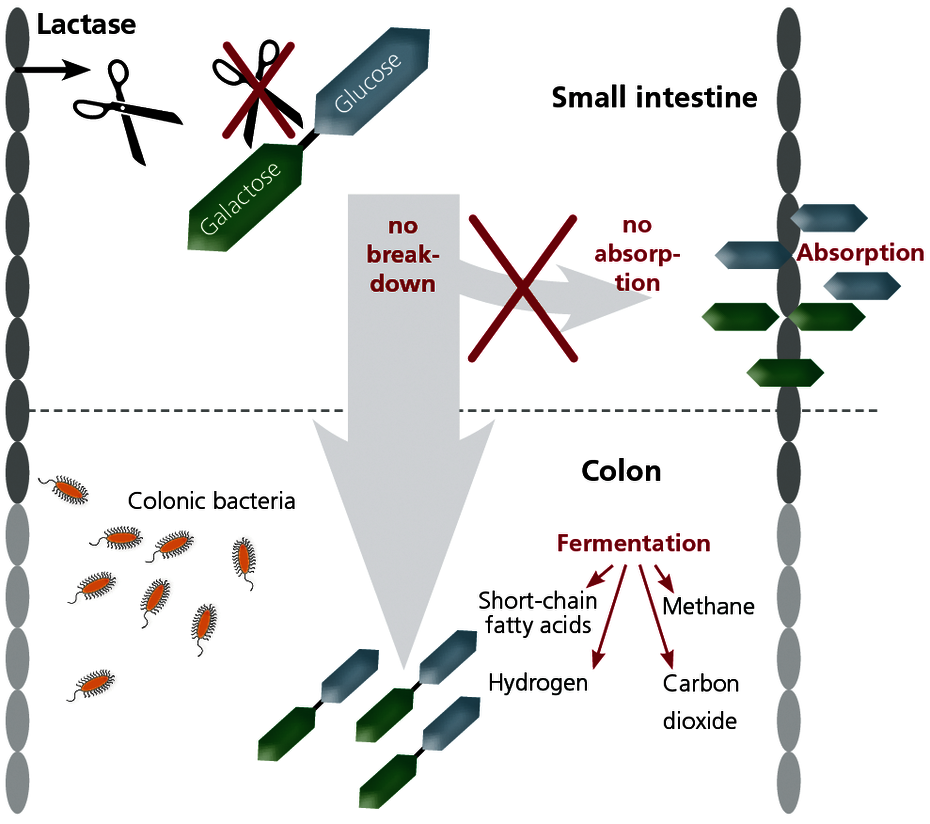
Normally the disaccharide lactose contained in food is broken down in the small intestine. The enzyme lactase formed in the small intestine splits the lactose into its constituents galactose and glucose. Only these monosaccharides can be resorbed separately through the wall of the small intestine.
In the event of a lactase deficiency, the lactose molecule does not split and cannot be resorbed. As a result, the lactose ends up in the colon undigested, where it is fermented by the intestinal bacteria. Lactose intolerance is thus due to an enzyme deficiency and must not be confused with a milk allergy, where the immune system reacts to components in milk.
Symptoms
The bacterial lactose fermentation products (CO2, short-chain fatty acids, hydrogen and methane) in the large intestine lead to symptoms such as sense of fullness, bloating, meteorism (drum belly) and convulsive stomach pain. The remaining lactose molecules are osmotically active and therefore in many cases cause diarrhoea. The reduced absorption of glucose in the small intestine can also temporarily induce hypoglycaemia bringing about symptoms of fatigue and lack of concentration.
Primary (adult) lactose intolerance is the most common enzyme deficiency worldwide and is genetically determined.
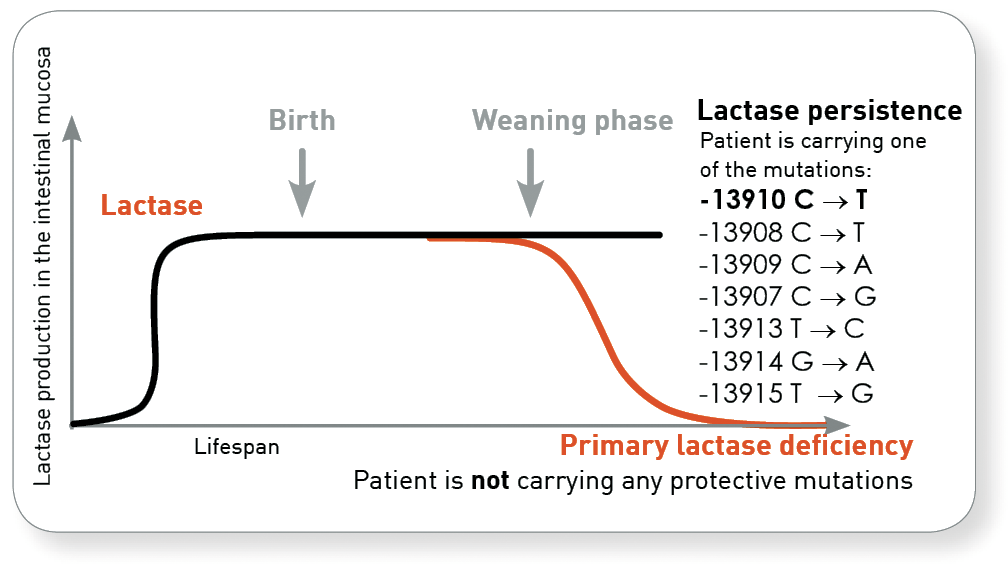
As with all mammals, the production of lactase in humans decreases after weaning through withdrawal of the mother's milk. In populations that carry out intensive dairy farming, protective mutations developed approximately 7,500 years ago, ensuring lifelong lactase persistence for the mutation carrier. Even now, however, not everyone has such a genetic variant important for lifelong dairy digestion. For these people, lactase production continues to decrease throughout their life. This explains why those affected can tolerate dairy in childhood, but that symptoms then gradually develop.
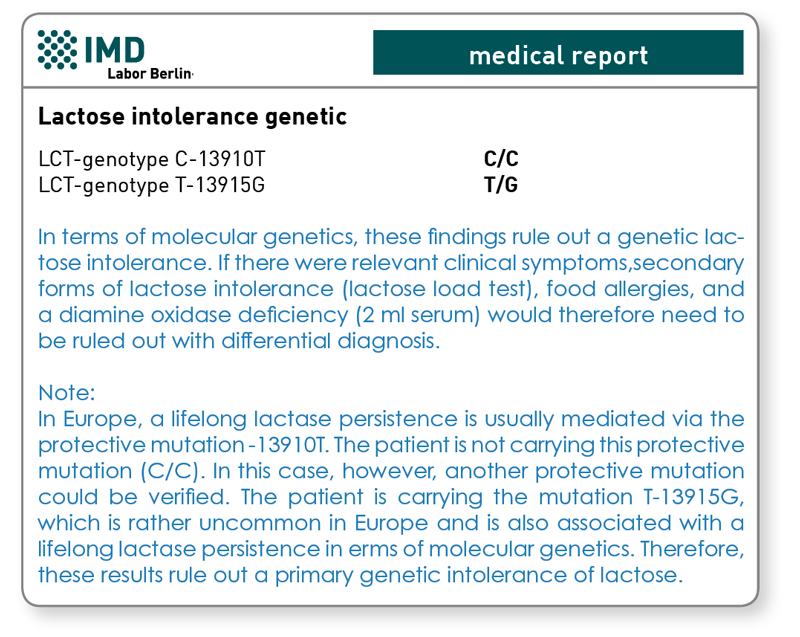
In Europe, as an adaptation to the lifelong consumption of lactose, a cytosine (C = decrease in lactase production) at the position -13910 in the lactase gene in the DNA has been exchanged for a thymidine (T =lactase persistence). A gene test can detect whether this protective gene variant is present or whether there is a predisposition to primary adult lactose intolerance. Approx. 75 % of the German population has this protective gene variant, which is why the test has been established in Germany when primary adult lactose intolerance is suspected.
The genetic test also includes rarer protective mutations.
Today, we know that the figure of 25 % affected was overestimated, as the mutation -13910 C → T that is usually investigated is not solely responsible for the persistence of lactase production. In parallel with the development in Europe, an adaptation to the lifelong consumption of lactose has taken place in other regions also. Other genetic variants in the lactase gene associated with lactase persistence are the polymorphisms -13907 C → G, -13913 T → C, -13914 G → A and -13915 T → G.
These genetic variants appear after all in approximately 10 % of cases that are examined in our lab. These additional mutations are therefore also present in the German population. That has induced us to change the analysis technology to the ultramodern DNA sequencing. Therefore, all responsible mutations are now detected unequivocally. As a consequence, a (further) protective mutation can be determined for an additional 10 % of the patients.
With the secondary form of lactose intolerance, the production of lactase is not reduced because of genetics but as the result of another underlying condition.
A secondary lactase deficiency can manifest itself in damage to the epithelium of the small intestine (the place where lactase is synthesised) e.g. when cytostatic or antibiotic treatment is given, or with patients who have coeliac disease or Crohn's disease. Lactase deficiency with a secondary cause is only temporary and is reversible after the intestinal epithelium is regenerated. The lactose load test is used diagnostically to verify a current lactose intolerance. With the corresponding clinical symptoms the lactose intolerance genetic test is offered as an easy lab test alternative that gives the patient no discomfort, since lactose loading of the patient is omitted. Collection time and concomitant diseases do not affect the test either. In addition, the genetic testing can be used to differentiate between primary and secondary lactose intolerance. The lactose intolerance genetic test is therefore recommended as follow-up testing in the case of all positive results in the lactose load test.
Only the genetic test can differentiate between primary and secondary lactose intolerance
The difference between genetically determined primary and secondary lactose intolerance is of great therapeutic importance because for patients with the primary form of lactose intolerance the only possible treatment options are a lactose-free diet or a diet low in lactose, or else to take lactase preparations for life. For patients with a secondary form of lactose intolerance, however, this treatment is only necessary until the intestinal epithelium has regenerated, following clarification of the cause and treatment of the underlying disease. A lifelong lactose-free diet is not necessary in the case of secondary lactose intolerance.
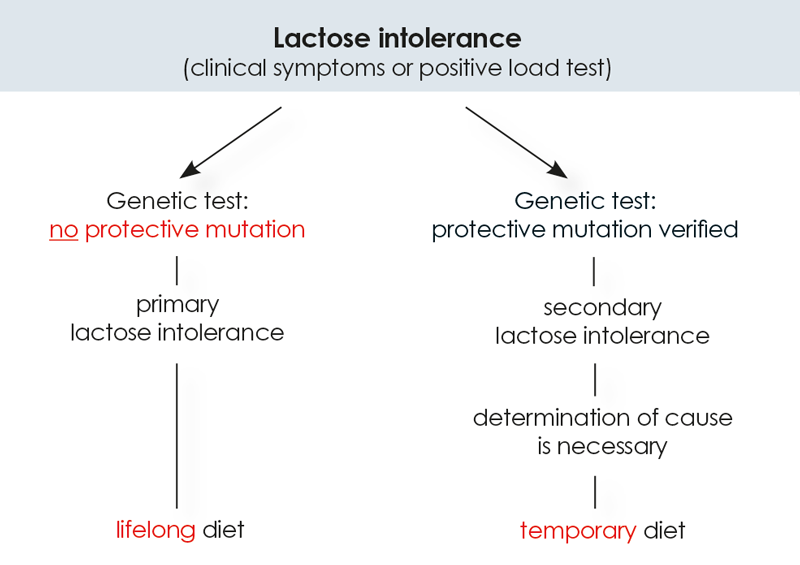
Fig. Only the genetic test can differentiate between primary and secondary lactose intolerance. The method used at IMD also detects the rarer “protective” genetic variant.
Material
2 ml EDTA blood
Transport to the laboratory is not time critical and can be done by mail.
Invoicing
Please obtain the costs for the analysis from the pdf-document.
Genetic testing for lactose intolerance - an alternative to previous test procedures
|