LTT - Immune Function
Use of LTT in immune function testing
The lymphocyte transformation test (LTT) was first used in the early 1980ies; at that time exclusively to study the immunocompetence of T helper cells. Twenty more years had to pass before allergy and infection testing were added to its indications.
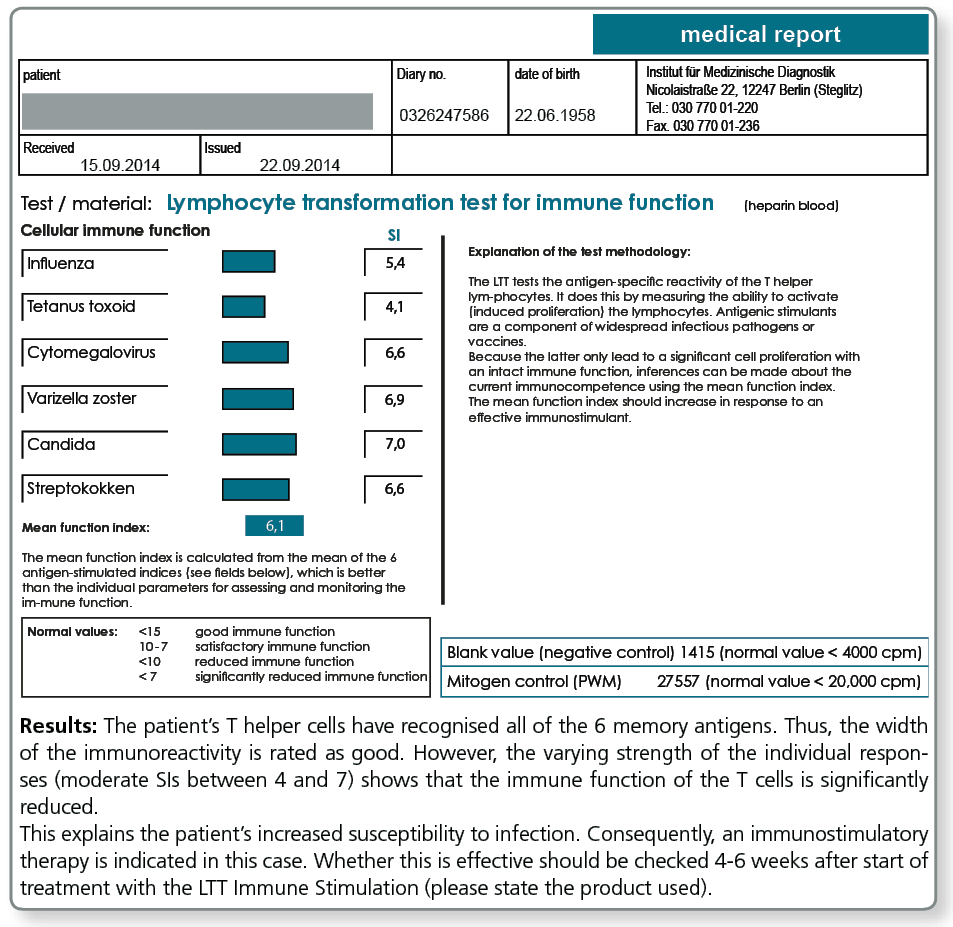
Over the years, LTT Immune Function (LTT-FU) has developed into a method capable of providing quantitative measurements of the functioning of immune cells extracted from blood. The basic principle underlying the test is to stimulate lymphocytes by exposing them to components of common pathogens or vaccines. These represent memory antigens which should trigger a strong immune reaction in people with a healthy immune system. When the LTT is performed, these antigens are first prepared by monocytes and dendritic cells and then presented to T helper cells. The specific T cells are activated and stimulated to divide, subject to the current state of immunocompetence. Quantitative measurements of DNA synthesis which always goes along with cell division are then performed. Strong activation in the LTT is indicative of intact immune function. It is also possible to use the LTT to monitor immune function over time. In this way it can be checked whether an improvement in the immune function has been achieved by immunostimulatory treatments (therapy monitoring).
The LTT Immune Stimulation is more extensive compared with the LTT Immune Function. With this test, selected immunogenic immunostimulants are tested in addition to the 6 memory antigens.
Especially when used for therapy monitoring, the LTT Immune Stimulation helps to individually select suitable immunostimulatory products or to detect early on any loss in efficacy (see here).
Clinical cardinal symptoms of a cellular immunodeficiency include:
- Reduced resistance to infection
Mainly against viruses, persisting intracellular bacteria and yeasts (Candida) with primary manifestation at the mucous membranes of the upper respiratory tract and the intestines. - Significantly prolonged convalescence after acute infections
- Wound healing disorders
- Reduced immunocompetence against tumour cells
Cellular immunodeficiencies can be congenital (primary immunodeficiencies, some with late manifestation at an advanced age) or secondary to an underlying disease, such as malignancies, chronic inflammatory conditions, infections (not only HIV!), or immunosuppressive treatment (secondary immunodeficiencies).
The most common causes of secondary cellular immunodeficiencies in patients with chronic inflammatory diseases is the impact of the systemic inflammation on the immune system itself. These can be triggered or promoted by malnutrition and unhealthy eating habits, chronic stress, allergic conditions and chronic persistent infections.
The interaction of the endocrine system, the nervous system and the immune system make the immune defence against pathogens and also tumour cells so complex that it is difficult to assess.
Without advanced cellular immune function tests it is impossible to obtain quantitative measurements of the severity of immune function disorders, especially as the Mérieux multitest has been taken off the market because of its low reproducibility.
Today, effective immunomodulatory treatments are available. Therefore, high-quality qualitative tests are of utmost importance to support the selection of adequate treatment options and to monitor efficacy.
Indications for the LTT Immune Function (LTT-FU)
- Increased susceptibility for infections / Frequent acute or chronic infections
Mainly caused by viruses, persisting intracellular bacteria and yeasts (Candida). - In cancer patients
To determine the functional immune status before and after surgery or chemotherapy and radiotherapy as well as over the course of immunostimulatory treatments. - In chronic inflammatory diseases
To assess the secondary immunodeficiency resulting from systemic inflammation. - In HIV infection
To determine the current immunological status, before and over the course of antiviral therapy (evidence of restoration of a functional immune system). - Where immunodeficiency is suspected
due to malnutrition (vitamin, zinc, protein and iron deficiency).
What sampling material is required?
20 mL heparin blood and 5 mL whole blood.
Please request the collection material (LTT blood collection set) from the laboratory free of charge: Fon: +49 30 77001-220, Fax: +49 30 77001-236, E-Mail: LTT@imd-berlin.de
No more than 24 hours must elapse from the time the blood is collected to the time of receipt of the sample in the laboratory. During this time the blood samples should be stored at room temperature. We offer a free nationwide courier service.
Blood samples for cellular function tests should not be stored in the fridge!