Histamine intolerance
The clinical picture of histamine intolerance (HIT) is characterised by histamine levels exceeding a person’s histamine tolerance threshold. It is usually caused by a deficiency of the histamine-degrading enzyme diamine oxidase (DAO). The lack of a DAO can have primary (genetic) or secondary causes.
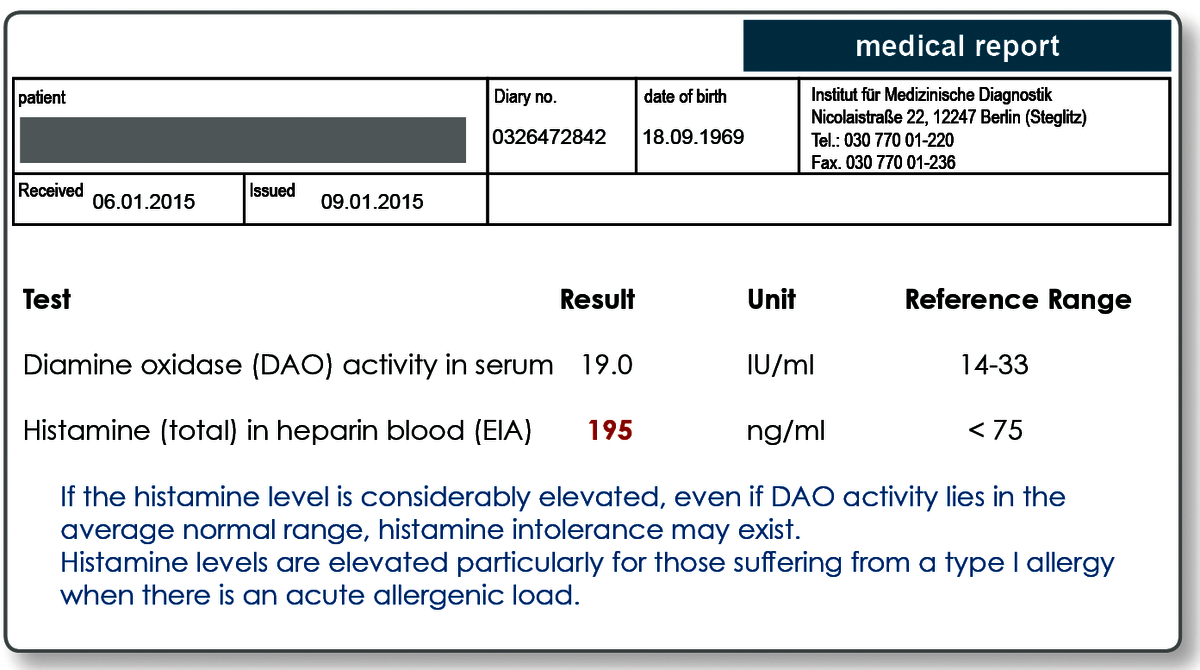
HIT can also manifest itself clinically if the body is loaded with so much histamine that, despite normal activity, the DAO cannot adequately metabolise this histamine. The excess histamine may be exogenous in origin (through ingestion with food) or it may be due to excessive levels of endogenously produced histamine (mast cell-associated inflammation, allergy). Both DAO deficiency and excessive levels of histamine can be determined with laboratory tests. In addition, a genetic test can be used to differentiate between primary and secondary DAO deficiency.
Histamine is the major mediator of allergic and pseudo-allergic reactions.
Histamine is a biogenic amine that is stored in mast cells and released when these cells are activated. As a vasoactive mediator, histamine plays a dominant role in allergic conditions such as allergic rhinitis (hay fever), allergic bronchial asthma and urticaria. Furthermore, histamine is involved in so-called pseudo-allergies to drugs and food additives, among others. In addition to the histamine released from mast cells in allergic processes, other histamine enters the body through the ingestion of food.
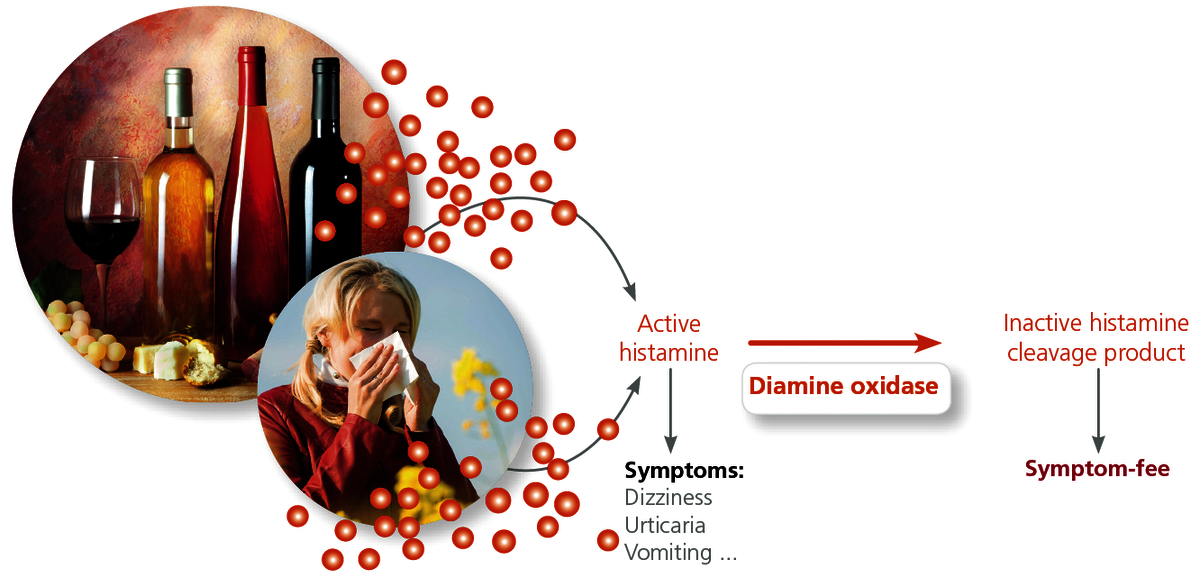
The enzyme diamine oxidase (DAO) is the key enzyme responsible for the degradation of histamine.
DAO enzymatically degrades extracellular (free) histamine regardless of whether the histamine originates from allergy-induced processes in the body or is consumed with food. It is degraded to imidazole acetaldehyde which, after methylation as a methylhistamine, is eliminated via the kidneys. The activity of DAO determines the rate of histamine degradation. If the activity of DAO is inhibited, histamine will accumulate in the blood. The second histamine-degrading enzyme, histamine N-methyltransferase (HNMT), only breaks down intracellular histamine, and is thus only of minor importance for HIT.
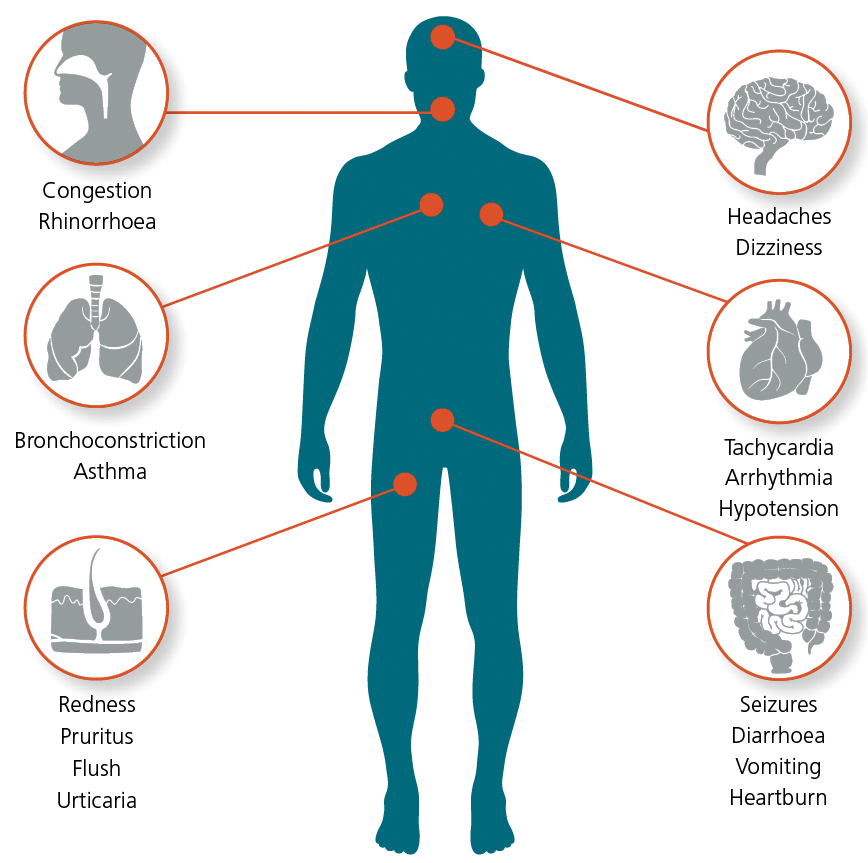
The symptoms of histamine intolerance (HIT) vary.
Since histamine receptors are located nearly everywhere in the body’s organ systems, HIT symptoms are highly heterogeneous. Main symptoms of HIT are flush, diarrhoea, nausea, headache, hot flushes and shortness of breath. Eczema, rhinitis, episodes of urticaria, hypertension, colitis, asthma, and malaise may also occur. Typically, there is also an intensification of symptoms with a concomitant IgE-mediated type I allergy to substances including pollen, mould, food, or insect toxins.
HIT can "fake" a food intolerance.
Histamine is present in food, where it is primarily produced during maturation and fermentation processes. Bacterial enzymes (decarboxylases) convert the histidine in food to histamine. This means the longer food is stored, the greater its histamine content. Histamine is heat-stable and cannot be destroyed by common methods of food preparation such as freezing or heating. Because bacteria are responsible for histamine formation, large amounts of histamine are found in microbially produced or fermented foods (cheese, sauerkraut, wine) as well as in high protein foods such as fish and meat. If the activity of DAO is inhibited, the histamine degradation capacity is severely reduced, which is why consumption of foods that contain high levels of histamine can lead to the previously mentioned intolerance reactions.
DAO activity and histamine concentration in the blood can be measured.
DAO is stable and is continuously released into the bloodstream. The activity of the DAO in the serum correlates with the histamine degradation capacity of the body and therefore represents a suitable marker for the diagnosis of HIT and HIT-associated disease patterns.
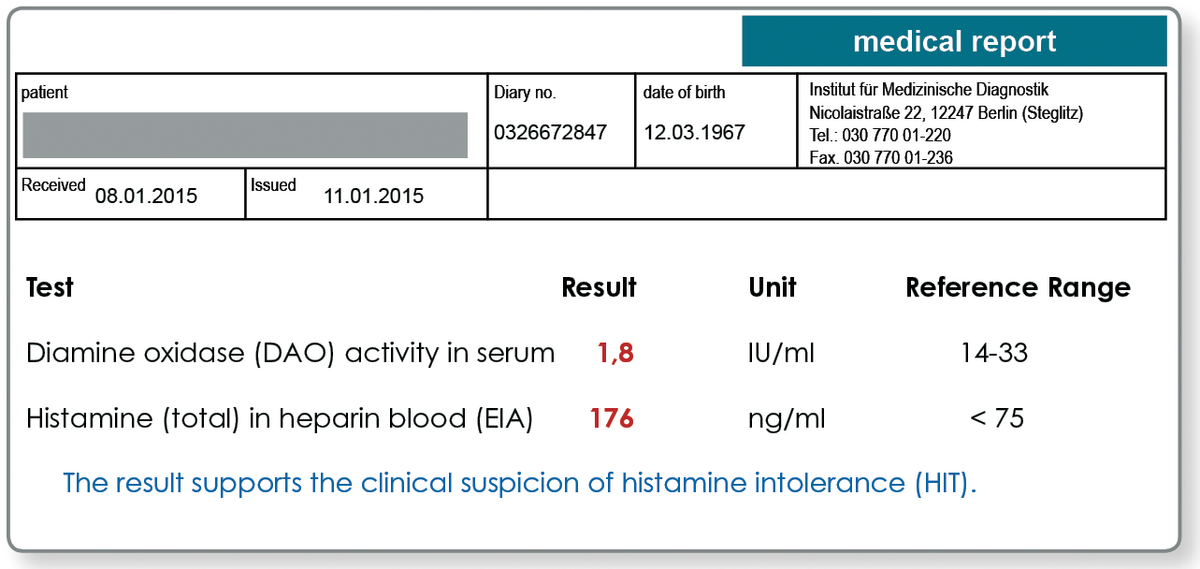
HIT can develop, if histamine from the ingestion of food or released in an allergic response is insufficiently degraded due to DAO deficiency. Histamine intolerance may also clinically manifest if there is an excess of histamine that "overwhelms" the normal DAO activity. Allergic disorders, such as hay fever or sensitisation to mould or other allergens, are additional elicitors of histamine and can have an additive effect to the histamine from the ingestion of food. To determine if the individual tolerance threshold has been exceeded, DAO activity should always be analysed at the same time as the total histamine concentration in the blood.
The histamine N - methyltransferase ( HNMT ) is irrelevant.
Apart from the oxidative deamination by diamine oxidase ( DAO ) Histamine can be degraded by a second mechanism in the body , namely by ring methylation by histamine N - methyltransferase ( HNMT ) . The DAO is as a secretory protein responsible for the degradation of extracellular histamine , whereas HNMT is only present intracellularly , mainly in the liver . Therefore, only the DAO plays a crucial role for the breakdown of ingested dietary histamine.
The genetic test can differentiate between primary and secondary DAO deficiency.
To avoid unnecessary lifelong dietary restrictions, in the case of an existing DAO deficiency, it subsequently needs to be established whether this deficiency of DAO is primary (genetic) or secondary, because the result has other therapeutic consequences.
In primary DAO deficiency, certain sequence variants (polymorphisms) in the DAO gene lead to a significantly reduced DAO enzyme activity. These genetic variants can be detected in laboratory tests. This genetic test is primarily indicated in patients with confirmed low DAO activity and associated clinical symptoms in order to make a differential diagnosis between a primary (genetic) and a secondary (and thus usually reversible) form of histamine intolerance.
Inflammatory or degenerative bowel diseases are a common cause of temporary secondary DAO deficiency, as more than 90% of DAO is produced from the intestinal epithelium. Inhibition of DAO activity as a result of the action of medications, alcohol or toxins is also referred to as a secondary form of HIT. Known "DAO inhibitors" are listed on page 20. However, many newer drugs have not been tested in this respect. Copper deficiency is another possible cause for reduced DAO activity, as copper is a central atom of the DAO and thus essential for it to function.
| Acetylcystein | Cefotiam | Dobutamin | Pentamidin |
| Alcuronium | Cefuroxim | Isoniazid | Pethidin |
| Alprenolol | Chloroquin | Metamizol | Prilocain |
| Ambroxol | Cimetidin | Metoclopramid | Propafenon |
| Amilorid | Clavulansäure | Metronidazol | Thiopental |
| Aminophyllin | Cyclophosphamid | Morphin | Thiamin |
| Amitriptylin | Dihydralazin | Pancuronium | Verapamil |
Tab: Selection of DAO-inhibiting drugs
Therapeutic consequences of low DAO activity
If reduced DAO activity or elevated levels of histamine are detected, foods that contain high levels of histamine must be avoided. If a secondary form of HIT is present, i.e. reduced DAO activity despite a normal genetic makeup, the cause should be investigated (chronic inflammatory bowel disease? copper deficiency? prescription drug and alcohol history?) as, in contrast to the primary form, secondary histamine intolerance is usually reversible.
Because copper is essential to DAO function, copper levels should be monitored in patients with low DAO activity to avoid further deterioration of the remaining DAO activity through copper deficiency. Zinc levels should be checked at the same time, as zinc prevents intestinal copper absorption.
Symptomatic treatment through administration of H1-receptor antagonists should only be a temporary measure.
Material
Determination of DAO activity: 2 ml of serum
The laboratory test used detects the activity of the DAO enzyme. The DAO ELISA test used in some laboratories, on the other hand, measures only the DAO concentration and is therefore inadequate for verifying the secondary form of HIT.
Total histamine in blood: 10 ml heparin blood
Both tests can be kept at room temperature and sent by mail within 24 hours, but it is recommended to send them in by courier.
DAO genetic testing: 2 ml EDTA blood
Transport of the blood sample to the laboratory is not time critical and can be done by mail. For genetic testing, we require the signed consent of the patient.For further questions please contact us by phone at 030 77001 220.
Literature
- Maintz L., Novak N: Die verschiedenen Gesichter der Histaminintoleranz, Deutsches Ärzteblatt 2006; 103/51: 3477-3483
- MusiK E. et al. Serum diamine oxidase activity as a diagnostic test for histamine intolerance. Wien Klin Wochenschr (2013) 125:239–243